
Conditions That Are
Hostile to Life
At its very conception, pollutants were introduced into this country’s soil: settler colonialism, anti-Black racism, white supremacy, racial capitalism, and heteropatriarchy, at just the beginning of the list.
The foundational atrocities of colonization and slavery at the center of the United States’ own birth story are but the first sign of contamination. Having thoroughly infiltrated our society and our systems, these toxins persist today, the effects of which are visible in who is most likely to suffer abuse during childbirth, to who has the opportunity to attend midwifery school, to who receives funding to open a birth center. Poisoning our communities and our ability to provide our communities with necessary care, these pollutants have created an environment that is utterly hostile to life.
Shaping and influencing the ecosystem birth justice actors must navigate, there are specific ways in which these pollutants show up in our work that create conditions that are hostile to birth justice. Manifesting as persistent settler colonialism, persistent racism, delegitimization of care work, financial instability, burnout and moral injury, internal conflict, and entrenched power, these conditions are existential crises that undermine the potential of the birth justice movement.
We describe these conditions discretely in order to see their elements more clearly, but many of us are impacted by several or all of them at once (similar to the multilayered experience of oppression described by intersectionality). For example, the way midwives of color are forced to suffer racism dealt indiscriminately by midwifery educators, fellow midwives, professional associations, and clients is a particular form of violence and trauma that is a combination of the effects of settler colonialism, racism, delegitimization of care work, internal conflict, and entrenched power.
As you move through this section, we invite you to take inventory of how these conditions show up in your own work. While some of us have already begun answering this question, we call everyone in the birth justice movement into proactively considering how we might prevent or mitigate the effects of these conditions (and remediate our soil to eliminate the causes), so we can give ourselves the best fighting chance.
“While I was apprenticing with that white midwife, I went through some of the most racist, uncomfortable experiences in her birth center.
It was located 35, 40 minutes from where I lived in the suburbs. It was mostly upper middle class white women, and they were extremely rude.
They were cringing, drawing back,
even if I wanted to take their blood pressure.”
—Okunsola M. Amadou


Settler Colonialism
Settler colonialism, the founding toxin of the United States, persists today such that it continues to create conditions that are antithetical to birth justice’s visions of liberation. The land upon which we all live and conduct our birth justice work remains land that was stolen from Indigenous peoples through genocide, and this atrocity has not been accounted for through compensation, legal or political redress, or even widespread cultural acknowledgement. Because this system ensures that we all benefit from its control and exploitation of the land in some way (including those who are also oppressed by other systems), it also ensures its own maintenance and replication.
What’s more, the settler-colonial tools used to enact this theft are still in use today, including the Western European legal system. While efforts led by Indigenous peoples have been made to mitigate the danger of these tools, or transform them, dangers remain. Evidence of those efforts and the remaining dangers includes the very fact that many of the peoples who originally inhabited this land are still here, practicing resistance and liberation, while experiencing inequities in perinatal health.
Additional effects of settler colonialism on the United States in general, and on the field of birth justice in particular, involve multiple ongoing forms of violence. This includes sexual violence and violence against the land, which encompasses the exploitation of natural resources; air, water, and nuclear pollution; and climate change. This violence threatens all of Earth’s ecosystems and its inhabitants, including us. Genocidal violence is always a threat to birth justice.
Racism
So pervasive and influential has racism been in the shaping of our society that its past manifestations have had resounding effects on the present. Gynecology and obstetrics’ roots in experimentation on enslaved Black women’s bodies directly contributes to the harm physicians and nurses inflict upon Black birthing people today. The ousting and outlawing of traditional midwifery in the early 19th century directly contributes to the obstacles Indigenous, Black, and other midwifery students of color face when trying to enter the profession today, as well as the overall stigma midwifery and community birth must now overcome. The accumulation of wealth for only the most privileged identities under racial capitalism, an economic system built on colonization and anti-Black racism, produced a philanthropic model that we often rely on for funding even though it was designed to reconstitute white supremacy. Flowing out of the very culture that surrounds us, racism rears its ugly head everywhere we fight for birth justice.
Interpersonal racism is rampant, and while people of all races inflict racialized harm, white women have been particular culprits and have posed explicit barriers to the efforts of Black women. People of color (itself a monolithic term that is simultaneously used for our solidarity and division) are gaslit about our experiences and flattened into a singular identity. Black and brown people are dehumanized, our bodies still used for experimentation and as repositories for sexual violence and environmental contamination. We are intentionally barred from accessing quality care, education, funding, and power. And of course, Black women and birthing people bear the brunt of the maternal mortality crisis. Myriad more manifestations of racism litter this ecosystem.
To ignore or deny the racism at the heart of the perinatal health crisis is a clear demonstration of a lack of understanding of the problem and a lack of genuine commitment to the visions of birth justice. To ignore or deny its existence in our movement spaces will beget continued harm and rupture in spite of our aspirations to work together.
Delegitimization of Care Work
In Seeding Liberation, we describe a major strategy of the birth justice movement: manifesting the world we want to live in [Manifesting the world we want to live in], which entails creating spaces in our communities in which our people are centered and empowered. Worthy and visionary as this strategy is, however, the two prevailing tactics for activating it—growing the midwifery workforce and opening birth centers—are hampered by the delegitimization of care work.
At the heart of manifesting birth justice is “care work:” the labor of attending to others’ needs. Much of birth justice work (including, but not limited to, midwifery and doula care) is “care work,” but care work has been structurally and systematically delegitimized in our society.
In a country where, for centuries, much of the care work was done by enslaved Africans and their descendants, it is absolutely no coincidence that today, care work is done primarily by women of color. Over 90% of domestic workers are women. Black, Hispanic, and Asian American and Pacific Islander women are vastly overrepresented among this workforce. Unpaid “family work,” such as care of dependents and households, is still largely performed by women. Flowing out of the dynamics of colonization and slavery, this formation of the care workforce is a continuation of the exploitation of gendered and racialized bodies in support of capitalism. In order for care workers to remain uncompensated (or compensated as little as possible) for doing work that enables others to do work that is profitable, white supremacy and capitalism must delegitimize their labor.
If our societal structures are designed to subjugate care work, then of course the infrastructure around it is inadequate [Financial Instability].
Nonetheless, some endeavor to enter the field. Would-be midwives encounter their first obstacle with midwifery education. Midwifery school is expensive and for CPMs, there is no financial aid. Many students must work concurrently (significantly extending the length of the program) or take on debt to make it through school. For those who do, more challenges lie ahead. This is not an accident.
Midwives across the board suffer from intense burnout [Burnout & Moral Injury]. The CPM payment model, in addition to providing wholly insufficient salaries, prevents them from taking time off. 30% of CNMs do not apply for relicensure after 5 years (ACNM, 2023) and, while the attrition of CPMs is not tracked, it is anecdotally similar. CPMs and CNMs alike grapple with inadequate and restrictive regulations that are inconsistent across states.
This care work is so devalued as to be vulnerable to every attack. There are few protections, buffers, or barriers. Structures that are supposed to be supportive often betray or disappoint us. It is no wonder that birth justice actors, especially birth workers, find ourselves feeling uncared for and unable to afford doing the work of caring for others. Under these circumstances, the pathways to becoming a midwife are toxic and the cumulative effect of staying a midwife is doubly toxic.
The toxic dose from becoming a doula is less potent, but constant exposure to toxicity produces similar challenges to staying a doula. Most doulas work in hospital settings where they are constantly exposed to obstetric violence and racism. Operating under a fee-for-service model like CPMs, they likewise struggle to make a living wage.
Those looking to start birth centers encounter their own obstacles (which only add insult to injury for those who are midwives). As with midwifery, the start-up costs are often the insurmountable obstacle, especially for projects led by Black folks and other people of color, on tribal land, or serving Indigenous people. Layered on top of this are the policy hoops to jump through at multiple levels of government (think building codes and state certificates-of-need). Once the birth center is open, the existing reimbursement model makes the dance of expenses versus revenue a constant nightmare.
In order to successfully implement our strategy of manifesting the world we want to live in, we must see birth justice as a direct challenge to the entire architecture of laws, policies, and systems functioning to make care work invisible and undervalued. Without this structural change, we run the risk of burnout and the false appearance that these models of care don’t really work.
American College of Nurse-Midwives. (2023). ACNM Workforce Study Data Brief No. 1: What is the rate over time that midwives leave clinical practice? (Report No. 1). https://www.midwife.org/data-briefs


-
A De Facto Ban
“We're still working to get home birth insurance coverage. Ironically, we've had a law on the books now for five years finally licensing CPMs, but even the state that signed the law allowing them to practice does not cover home birth for their own employees. So it's still a de facto ban.”
—Michelle Drew
-
Care for the Caretakers
“Take care of midwives, take care of doulas, take care of Black maternal health providers and leaders. The more exhausted and burnt out and trauma-filled we are from seeing traumatic birthing experiences, the more we're going to lose valuable people.”
—Okunsola M. Amadou
-
Fight for Fair Payment
“Right now, one of the primary issues is payment and fair payment. When I'm within the hospital system, there is a law that mandates that insurance has to reimburse me equally to a physician when they're providing the same services. However, if you decide to go to the local birth center or if you're choosing a home birth, they are not reimbursed at all.”
—Michelle Drew
Financial Instability
In What Seeds Need [What Seeds Need], we establish the analogy that water is to seeds as funding is to birth justice actors: an essential resource needed to propel and sustain our work. The reality is that our fields lay dry, our coffers sit empty, and even when briefly replenished, the underlying drought conditions remain. This drought is not a natural occurrence but a consequence of our societal structures, steeped in interlocking systems of oppression, creating an unequal distribution of resources. As a result, our movement is dismally underfunded at both an individual and organizational level.
The individual level

Few participants in our survey, interviews, and murmurations felt that they are sufficiently compensated for their work. 63% of our survey respondents indicated that their income does not cover all of their expenses. It’s alarming that despite the attention to the perinatal health crisis, framed as the bellwether for health inequities and systemic racism in the US, the majority of those driving changes and improvements do not meet their cost of living.
Unsurprisingly, those whose income does not equal a living wage are mostly doulas, midwives, organization staff, and entrepreneurs. As Michelle Drew notes, “If you’re a direct service birth worker like a midwife or doula, your reimbursement rates are probably not enough for you to sustain your family.” And while some movement members expressed that their cost of living is covered, we are concerned that this work might only allow us to survive and never enable us to thrive. Few of us have benefits—healthcare, retirement, and paid time off to name only the most basic. Cobbling together program-specific grants to do the work itself, and channeling all revenue into the success of the enterprise, rarely leaves money on the table for benefits for organization staff and entrepreneurs.
Most birth workers derive their income from a fee-for-service model that requires them to work every week of the year. (Not to mention that many are pulling double duty, trying to secure policy change in their spare moments, which is often unpaid work.) The effects of this payment model are exacerbated by the fact that most individuals who hire birth workers—those often impacted by the intersections of race and class—are unable to pay the full cost of a doula or community-based midwife. Offering no reprieve, many donors refuse to fund direct services. This frequently leaves birth workers with the impossible choice between making their much needed services accessible and paying their own bills.
For those who choose not to make any income from their birth justice work, it may be a strategy to root care work in community and outside capitalist economic models. This datapoint, among many from our survey results, offers a jumping off point for further research into the many ways birth justice actors actively resist systems of oppression [Seeding Liberation].
The organizational level


Only 11% of survey respondents stated that their organizational costs are covered by their current funding. Given the millions of dollars of federal and private investment in improving perinatal health, it’s shocking that at least 75% of birth justice organizations lack sufficient funding. Funding for birth justice organizations often only narrowly covers specific programs or interventions and neglects the more imaginative solutions and systems change we propose as well as the costs of maintaining the organizational infrastructure that makes those programs and interventions possible.
Despite the lack of resources, many of us hold up our organizations through sheer will and creativity, and continue the work out of a refusal to give up on crucial systems change and the families who need care. We scrape together resources however we can, and too often rely on family and friends for financial support, which can be alienating and strain our most important relationships. It’s not uncommon for us to take on other full-time jobs (related to birth justice or not) to support our own birth justice work.
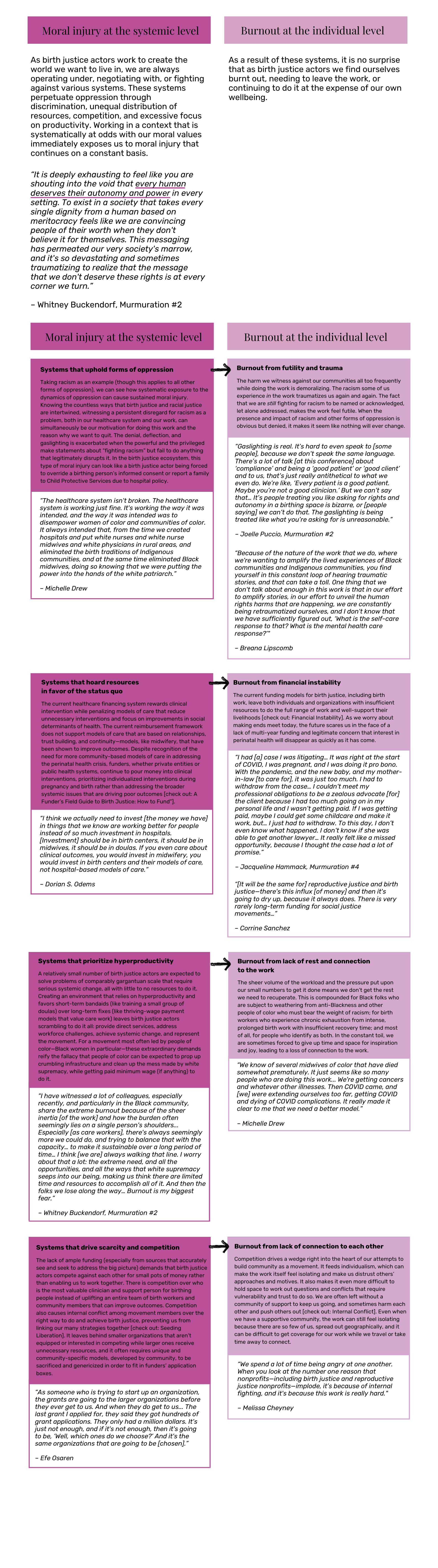
Burnout & Moral Injury
In our analysis of the dataset, it became abundantly clear that across the birth justice landscape, far too many of us are burnt out or well on our way there. And it’s no wonder… We’re expected to serve our communities; influence change in our local healthcare settings; advocate for policy change at all levels of government; mentor new birth justice actors; and inform donors, the media, and the general public on why this work is important and how to do it effectively—all while keeping our own families afloat and experiencing harm in the work.
Burnout is a state of complete physical, mental, and emotional exhaustion.
Moral injury refers to the lasting distress caused by actions that violate our core moral values. We can experience this distress from morally compromising actions at the individual, interpersonal, and social level. Often, however, these actions take place at the systemic level, wherein the systems in which we operate put us into morally compromising positions. Like other injuries, moral injury takes time to heal. Removing the source of the injury can allow for healing, but when the source of harm is pervasive and can’t be escaped, like when it is systemic, it can lead to burnout at the individual level.
Internal Conflict
As a social movement taking on systemic oppression, it is important to recognize the difference between fighting against that oppression and fighting with our own allies, whether “potential,” “problematic” or “proven” (see “Loretta Ross: ‘Don’t Let the Chain of Freedom Break at Your Link’” in Recommended Reading [Recommended Reading]). Propped up by the dominant systems and structures of our society, our opponents—individuals and organizations who oppose birth justice, whether as a stated stance or simply via upholding the status quo—already hold much of the power and resources, allowing them to define the rules of engagement and take advantage of the status quo. Our ability to confront these opponents and the systems of oppression they maintain is compromised by internal conflict—perceived or actual conflict or competition between individuals and organizations within the movement, i.e. those working toward birth justice.
This breakdown in connection has clear origins in the systems against which we struggle. Systems of oppression create the conditions for internal conflict. We are pitted against each other through a variety of mechanisms, from racial hierarchy under white supremacy to scarcity of resources under capitalism [Burnout & Moral Injury], only to name a few. Therefore, the existence of internal conflict in our movement is no one’s individual failure, and yet it often falls on individuals to solve. But it can’t be remedied alone or with a one-size-fits-all solution. Like all things birth justice, it requires a complex approach [Complexity].
However, if we, as a movement, cannot find ways to build bridges and nurture productive working relationships, whether with “potential,” “problematic,” or “proven” allies, on the ground, we will continue to cause each other harm and burn out, and the work will stall. In the grand scheme, the opposition will continue to have the upper hand.


Entrenched Power
With 363 responses from birth justice actors across the United States, collected from October to December 2023, though not a representative sample, our survey paints a picture of who we are as a movement and allows us to draw some important conclusions. Despite the fact that many of us, as with other social justice movements, strive to uplift the leadership of those most impacted by the problem, this picture illustrates the disconnect between those we seek to elevate and those whose positionality amplifies their power.
Positionality refers to how one’s perspective, role, and responsibility are determined by our identities. Positionality is a useful tool because it gives us a way to examine ourselves and a practice for reflecting on who we are in relation to others. As you review this demographic data we invite you to consider your positionality in relationship to the positionality of others in the movement.
Painting a picture with the data

A quarter of survey respondents identified as doulas, and another quarter as midwives. Most of the remaining half work in organizations or academic institutions while a smaller group are entrepreneurs, community organizers, other types of clinicians, government employees, and lawyers.
Taking a closer look at how race factors into professional role, we see that white respondents were 3.6 times more likely than Black respondents to be nurses, CNMs, CPMs, and academics (54% vs. 15%, respectively). Meanwhile, 20% of white respondents and 32% of Black respondents identified as doulas. These discrepancies show how the power dynamic skews overwhelmingly in favor of white birth justice actors despite the number of Black birth justice actors in the movement.

Over a third of survey respondents work alone, and almost another third work in small-medium organizations. Only 7% work in primary care facilities and 5% in hospitals.
Breaking this down further by professional role, we see that the vast majority of doulas in our sample work alone (68%), with most others working in small-medium organizations (20%). Very few work in large organizations, primary care facilities, or hospitals.
We see a similar pattern when we break type of organization out by race as well, with people of color largely operating alone or in small-medium organizations: 72% of Black respondents, 85% of Indigenous respondents, and 90% of mixed respondents indicated working alone or in small-medium organizations, compared to 56% of white respondents.
This lack of representation of both birth workers and people of color in mainstream healthcare institutions reflects a significant disadvantage in accessing power and resources for two (overlapping) demographics that are both essential to transforming our healthcare system into one that is safe and equitable. Furthermore, we know from our research that operating outside of institutions is a deliberate strategy many birth justice advocates are choosing for survival, safety, and thriving.
Our survey’s findings on the distribution of birth justice actors throughout the landscape—and what we know about the structural reasons underpinning it—challenge the wisdom of focusing investment on institution-based scalability. The survey data affirms that leveraging small organizations and independent birth justice actors is essential to realizing the potential of the birth justice movement.
What the picture shows us
Our sample shows us that the birth justice movement itself still very much reflects the U.S.’ broader dynamics of entrenched power. Amid a healthcare crisis that disproportionately harms people of color, we find that people of color continue to be marginalized in professions with little power and low income. Simultaneously, they are pushed to operate in independent organizations (because they have been prevented from entering mainstream spaces or made to feel unsafe or unwelcome in them), and must scrape together the resources and respect to tackle the larger system.
In order to ensure that those most impacted by the perinatal health crisis (and therefore those equipped with the most insight into solutions) can be active participants—leaders—in solving it [Choosing our leaders and accomplices wisely], entrenched power has to be uprooted. We must actively shift power. Those holding disproportionate power, including white accomplices, must cede it. Funders must redistribute resources to projects and organizations led by people of color and others from marginalized communities.